
{kind=link}

Picture this: a man in his 20s has contracted COVID-19, but he doesn’t know it. He heads to the shop for some supplies. He stands in the socially-distanced queue, uses hand sanitiser and enters the store. He is not wearing a mask. He unintentionally showers the room with infectious respiratory aerosols and droplets, pays for his groceries, and then heads home. This has probably happened dozens of times across the UK. Despite this, face coverings were only mandated in shops and other enclosed public spaces from 24th July, in yet another example of the government’s response being too little, too late.
Like other respiratory viruses, SARS-CoV-2, more commonly known as COVID-19, is transmitted through droplets and aerosols produced when an infected individual coughs, sneezes, talks or breathes. Intuitively, blocking these droplets with a face mask should reduce transmission. This simple contention, however, has been the subject of hot scientific debate, policy clashes and political culture wars. After making the case that face masks work, we will pick apart how the UK government’s response fits into the timeline of emerging evidence and global decisions.
Face masks have been part of infection control for over a century. They were first implemented to combat an infectious disease epidemic in 1910, when plague swept through Manchuria, China, killing 60,000 people. Surgical face masks were adapted and mass-produced for use by the general population by Wu Lien-teh, a young Malaysian physician sent from Beijing to control the plague. This innovative measure received global attention, and large-scale mask-wearing was soon pressed into service as part of the response to the 1918 flu pandemic.
Despite their long history as a public health measure, there was very little evidence on the efficacy of mask-wearing until a handful of studies were conducted between 2003-2012 in the context of SARS, seasonal flu and swine flu. Early in the pandemic, critics claimed that the evidence that masks prevent infection was insufficient to support their use being mandated or even recommended. Commentators in publications like the Spectator still hold this opinion1.
So, do face masks work? The short answer is yes, although the full picture is a little more complicated. The scientific consensus is that face coverings, including home-made cloth masks, probably have the ability to reduce the risk of wearers spreading infection to others, a characteristic called ‘source control’. However, masks may provide little or no protection to the wearers against contracting infection from others.
The evidence is by no means conclusive. Randomised controlled trials (RCTs) on wearing masks in the community suggest that face masks may have no significant effect. By contrast, observational studies comparing the number of cases in regions after introducing compulsory mask-wearing policies with their predicted infection curve have shown that large-scale mask-wearing appears to be effective[1-3]. Although it is difficult to disentangle this effect from other measures introduced around the same time or changes in population behaviour unrelated to mask-wearing, these studies support the intuitive rationale behind face coverings. Similarly, recent mechanistic studies investigating how well masks protect against droplets and aerosols in a laboratory setting show that even cloth face coverings significantly reduce the number of droplets and aerosols produced[4,5].
RCTs are considered the ‘gold standard’ of experimental design for assessing the effectiveness of a treatment. In these trials, subjects are randomly allocated to either a treatment group or a control group. Observational studies do not randomly allocate their groups but instead compare outcomes for people who happen to be given the treatment or not. Whilst care is taken to try and match the makeup of these groups to remove confounding factors, there is no guarantee that a hidden variable other than the treatment could be responsible for differences between the groups, and so evidence from these studies is less certain than equivalent evidence from RCTs. Nonetheless, policy decisions are routinely made based on observational data and indirect evidence in order to provide a timely response to a rapidly evolving situation. Sometimes, authorities need to follow the ‘precautionary principle’ and implement measures even if the evidence for them is inconclusive.
Whilst RCTs are the ideal standard of evidence to aspire to, they may underestimate the effectiveness of masks for several reasons. These include small sample sizes, low adherence to wearing masks in the treatment group, and wide variation in experimental conditions leading to significant heterogeneity in results. It is not possible to conduct an RCT to address this question on a large scale due to the obvious ethical difficulty of preventing subjects from wearing masks. They are particularly poor at evaluating source control, as this requires testing all individuals who come into contact with the subjects, and so many RCTs only measure personal protection.
One of the earliest voices to bring all this data together in support of mask-wearing in the community was Jeremy Howard, a data scientist from San Francisco, who released a narrative review[6] examining the available evidence on 13th April. He concluded that the evidence available in early April was strong enough to support mask-wearing in the community. Over 100 academics, including a Nobel laureate virologist, signed his subsequent letter calling for widespread implementation of mask-wearing. At the time, the US CDC recommended wearing face coverings only where social distancing was not possible while the WHO suggested that only symptomatic individuals should wear masks. Howard put this down to an excessive focus on personal protection as opposed to source control, the low supply of face masks, and a lack of evidence from RCTs overly influencing the recommendations of advisory bodies.
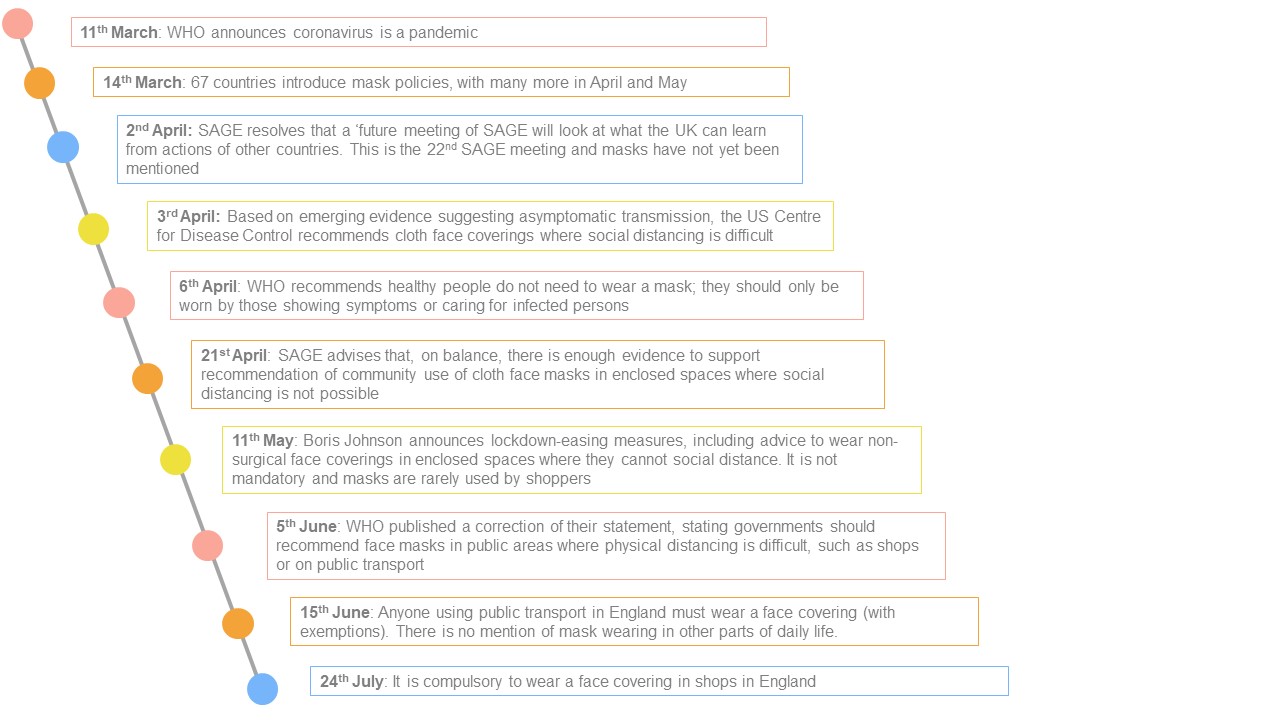
Developing evidence and conflicting advice from the WHO and the US CDC meant that masks were adopted much later than other measures (such as quarantines and social distancing) in many countries. Even taking this into account, the UK was still significantly behind the curve. Mask-wearing became compulsory in shops and on public transport in Vietnam, the Czech Republic and Austria in March. Germany followed suit by the end of April. In many countries in Asia, such as China, Singapore and Japan, masks were already so culturally embedded that mandation was unnecessary. The US CDC recommended wearing face coverings where social distancing is difficult on 3rd April, and the WHO updated their guidance on 5th June. Why was the UK government so late to act?
Using masks early in the pandemic posed a threat to supplies for healthcare workers. This was one of the key concerns identified by the UK’s Scientific Advisory Group for Emergencies, SAGE. This was not a surprise: an extreme shortage of PPE has been a strong theme in previous epidemics such as SARS. However, the response to this issue made little sense – instead of calling for increased production of medical and non-medical masks, the shortage was used as a reason to delay the recommendation of face masks.
Even once mask production caught up with demand, and evidence began to emerge that non-medical cloth masks could be effective, SAGE’s initial assessment was that the evidence for mask use in the community was ‘near nil’. This was mostly based on systematic reviews of RCTs[7,8] which showed no significant effect for masks.
Following reports to SAGE by the New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG)[9] and the Royal Society’s Data Evaluation and Learning for Viral Epidemics group (DELVE)[10], SAGE updated their guidance on 21st April to suggest that there was enough evidence to support ‘recommendation’ of community usage of cloth face masks in enclosed spaces where social distancing was not possible. It took until 11th May for the government to implement this, advising the public to ‘consider’ wearing face coverings in enclosed public spaces. It was perhaps unsurprising that this weak and unheralded recommendation was met with almost no response from the public.
Over the months of May and June, evidence continued to pile up. Reviews from the Royal Society[11] and the Lancet[12] sided with Howard’s earlier interpretation of the positive effect of mask-wearing. During this period, as noted above, more and more countries mandated the wearing of face masks. However, there was no mention of face masks in the SAGE meetings over this time period in response to the increasing consensus, and the low uptake of mask-wearing by the population. Only on 9th of July was a review of the policy to be scheduled.
The problems were summarised by SAGE member Sir Jeremy Farrar, who told MPs “I think there was not enough urgency… I regret that SAGE wasn’t more blunt in its advice and more robust. But it didn’t have a job in holding people to account, unfortunately, for delivery of interventions that were made.” Critical analysis of the government’s response was not regarded as within SAGE’s remit. This is a serious deficiency in the structure of our COVID-19 response framework, which fails to account for the possibility that politicians may misinterpret or misapply complex scientific concepts.
The uncertainty of the evidence and concerns surrounding PPE supply were key barriers to the widespread implementation of masks in the community, but the minutes from SAGE meetings show discussion of a wider variety of hypothetical problems. The general public might use masks until they become ‘soggy’. People might abandon hand washing and social distancing. New crimes, like mask theft, could emerge. Masks might add to people’s fear and anxiety. Rather than blocking mask policies, these concerns should have been used to inform a more effective campaign of messaging to the public.
Even when the evidence for face masks was considered ‘marginally positive’, there is an argument that they should have considered invoking the precautionary principle and recommended mandatory use. In a pandemic, we should be reaching for whatever tools we have, even if we’re not completely certain how well they work.
In the end, the government acted before SAGE had the chance to review their policy and make a stronger recommendation. They announced on 14th July that masks would become mandatory in enclosed public spaces, and this came into force on 24th July – yet another inexplicable delay.
Compare this slow action with how abruptly lockdown came into force. There is no public health rationale for this difference in approach. It appears, rather, that the primary concern of the government has been optics – they wanted to appear stern and decisive when the public concern about the pandemic was at its height, and now that we are growing weary of lockdown, they want to seem laid-back and unworried. Mr Johnson has done plenty of talking about the R number, but it is not difficult to imagine that he has been keeping a steady eye on his approval rating all the while.
Even now that we have finally caught up with the rest of the world on mask-wearing, its implementation has been half-hearted at best. The messaging that has trickled through to the population is ‘wear a mask, or pay the fine’. The full guidelines on the new mask rules were only released less than 12 hours before they came into force. This is simply inadequate.
Adverts and posters should be equipping the general public with an understanding of how droplets are transmitted, why masks should be worn, and the correct way to wear and dispose of them (see the resources below).
This will also affect how many people choose to comply. Without straightforward and comprehensive messaging, people may be left to gather information and make their own conclusions from sensationalist and highly-politicised sources. The anti-mask protests in the US, Canada and Germany may not be so far away as we like to imagine.
Mask-wearing was introduced too late due to fuzzy arguments, the dismissal of valuable observational and mechanistic evidence by SAGE and the slow implementation of their recommendations by the government. It is strange that mask-wearing was held to overly rigorous standards of evidence, when similarly intuitive non-pharmaceutical interventions such as coughing into one’s elbow, or socially distancing, were implemented with similar or lower levels of supporting evidence.
Of course, mask wearing is more unfamiliar and uncomfortable, and requires a proactive effort to increase production and supply of masks. But these are insignificant objections compared to the loss of life – and freedom – that our conservative approach to fighting this pandemic continues to cost us. Who said a pandemic was going to be comfortable?
Featured artwork by Arpita Chatterjee

Resources
Mask guidance:
Discussion of the evidence for face masks:
https://www.bmj.com/content/369/bmj.m1435
References:
1. Wang Y, Tian H, Zhang L, et al. Reduction of secondary transmission of SARS-CoV-2 in households by face mask use, disinfection and social distancing: a cohort study in Beijing. China BMJ Global Health 2020;5:e002794.
2. Wu J, Xu F, Zhou W, et al. Risk factors for SARS among persons without known contact with SARS patients, Beijing, China. Emerg Infect Dis. 2004;10(2):210-216. doi:10.3201/eid1002.030730
3. Lau J, Tsui H, Lau M, et al. SARS Transmission, Risk Factors, and Prevention in Hong Kong. Emerging Infectious Diseases. 2004;10(4):587-592. doi:10.3201/eid1004.030628.
4. Konda, A, Prakash, A, Moss, G et al. Aerosol Filtration Efficiency of Common Fabrics Used in Respiratory Cloth Masks. ACS Nano 2020; 14(5): 6339-6347 doi: 10.1021/acsnano.0c03252
5. Leung NH, Chu DK, Shiu EY, et al. Respiratory virus shedding in exhaled breath and efficacy of face masks (brief communication). Nat Med 2020; [Epub ahead of print.] doi:10.1038/s41591-020-0843-2 .
6. Howard, J, Huang, A, Li, Z, et al. Face Masks Against COVID-19: An Evidence Review. Preprints 2020. doi:10.20944/preprints202004.0203.v2
7. Brainard, J, Jones, N, Lake, I, et al. Facemasks and similar barriers to prevent respiratory illness such as COVID-19: A rapid systematic review. medRxiv 2020 2020.04.01.20049528; doi:10.1101/2020.04.01.20049528
8. Jefferson, T, Jones, M, Al Ansari, L, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Part 1 – Face masks, eye protection and person distancing: systematic review and meta-analysis. medRxiv 2020 2020.03.30.20047217; doi: 10.1101/2020.03.30.20047217
9. NERVTAG 2020. Wearing facemasks in a community setting: options and evidence. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/890233/s0150-wearing-facemasks-community-setting-options-evidence-160420-sage26.pdf (accessed 23 July 2020).
10. DELVE. 2020 Face masks for the general public. https://rs-delve.github.io/reports/2020/05/04/face-masks-for-the-general-public.html (accessed 23 July 2020).
11. Royal Society 2020. Face masks and coverings for the general public: Behavioural knowledge, effectiveness of cloth coverings and public messaging. https://royalsociety.org/-/media/policy/projects/set-c/set-c-facemasks.pdf?la=en-GB&hash=A22A87CB28F7D6AD9BD93BBCBFC2BB24 (accessed 23 July 2020).
12. Chu, D, Akl, E, Duda, S, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet 2020 395:1973–87 doi:10.1016/S0140-6736(20)31142-9
For Cherwell, maintaining editorial independence is vital. We are run entirely by and for students. To ensure independence, we receive no funding from the University and are reliant on obtaining other income, such as advertisements. Due to the current global situation, such sources are being limited significantly and we anticipate a tough time ahead – for us and fellow student journalists across the country.
So, if you can, please consider donating. We really appreciate any support you’re able to provide; it’ll all go towards helping with our running costs. Even if you can't support us monetarily, please consider sharing articles with friends, families, colleagues - it all helps!
Thank you!